
 07/11/2020
07/11/2020

In mid-May, Basma Issam felt a high temperature and shortness of breath. Within two days, her family members complained of the same symptoms. Basma, 24 years old, lives in an apartment in a suburb east of Cairo with her mother, her sister and her husband, and their baby daughter as well as her grandmother.
Two days after the symptoms appeared, she went to a private hospital for a chest CT scan. “At that point it was confirmed that my family and I had tested positive for COVID-19,” Basma told the reporter.
By July 13, 2020, the number of recorded Covid-19 cases in Egypt had reached 82,000. Since the announcement of the first case in mid-February, 3,858 had died from the virus.
After her diagnosis, Basma tried to find a place for her family in a quarantine hospital, but due to over crowdedness, Basma had to resort to home quarantine. Basma’s family is not alone in being forced to home quarantine –– ARIJ investigator documented the situation of 10 other families that were unable to secure beds in government hospitals.
Between 2005 and 2019, the number of government hospitals in Egypt decreased by 40.7% from 1,167 hospitals to a mere 691. Conversely, the number of private sector hospitals increased from 652 to 1,157, marking 77.4% increase, as reported in the health bulletin issued by the Central Agency for Public Mobilization and Statistics in 2019.
This investigation documents how the Egyptian government made a series of decisions that closed 476 government hospitals and shut down 60 specialised infection treatment hospitals or “Al Hemyat” –– that were better known in Egypt as “hospitals of the poor”. This happened at the end of the 1990s with the health reform plan, in which infection hospitals were transformed into mere departments in other major hospitals.
This decrease has left thousands of Egyptians unable to access adequate health care during Covid-19 pandemic, and what exacerbated the situation also is the successive increase in the cost of medical care, and the rise in the poverty rate to 32.5%, as reported in the income and spending statement issued by the Central Agency for Public Mobilization and Statistics for 2019.
Egypt bottoms the world’s healthcare index ranking at 84 out of 89 countries in terms of the level of healthcare provided to its citizens, according to 2019 data from CEOWORLD Healthcare Magazine.

Number of hospitals - Governmental sector
1167
691
 Decreased by
Decreased by

Number of beds - Governmental sector
116150
95683
Decreased by
the number of hospitals - Private sector
652
1157
 Increased by
Increased by
Number of beds- Private sector
18574
35320
Increased by
Dr. Muhammad Hassan Khalil is the general coordinator of the “Program to Defend the Right to Health”, (a healthcare rights organisation) , attributes the decline in the number of government hospitals to the privatization programs that the government has begun to implement.
In a phone call, he said that the health reform program launched by the Ministry of Health in cooperation with the World Bank in 1998 included the transformation of health services to become “profitable”, instead of being available at cost.
Khalil added that Dr. Hatim Al-Jabali’s tenure at the Ministry of Health from 2005 to 2011 marked a crucial step in privatization. It started with the attempt to privatize health insurance services in 2006 and continued with decision No. 637 to establish the Egyptian Healthcare Holding Company in the ensuing year.
Khalil explained that if it had not been for the court ruling issued in 2008 to stop the establishment of this company, the Egyptian health insurance assets would have been sold. After these plans were aborted, the government focused on another aspect of privatization by closing about 70 infection hospitals or “Al Hemyat” in February 2008.
This is in addition to the closure of about 500 “Takamol”, or integrated hospitals, established by the former Minister of Health, Ismail Salam, to serve as a link between primary healthcare units and central hospitals. This is all under the pretext of their low occupancy rates –– less than 25% –– and the lack of funding. According to Khalil, this is one of the reasons for Egypt's suffering during the Covid-19 pandemic.

Eight days passed in late May, and Basma Issam’s grandmother lost consciousness for more than 24 hours. During this time, Basma and her family searched relentlessly for a hospital to save her life.
After Basma gave up on finding a government ambulance, she was forced to hide her grandmother’s Covid-19 infection and contacted a private ambulance. However, when they saw her grandmother’s condition, they refused to take her down from her fourth floor apartment. Basma’s family was forced to carry this burden alone.
“I didn't know what to do or where to go with my grandmother,” Basma says. She decided to go to the Health Insurance Hospital in Naser City –– the closest to where they lived –– after it was dedicated to Covid-19 patients. However, because she arrived in a private ambulance, the hospital’s security officers refused to receive her grandmother.
Since 2010, management of Egyptian hospitals has changed. The Minister of Health, Hatim Al-Jabali, issued regulation No. 674 known as the “Unified List,” under which Egyptian hospitals were divided into six categories for the first time with a specified number of beds. This was unlike the previous regulation, No. 239 issued in 1997, which did not limit the number of beds in a single hospital.
According to the list, obtained by ARIJ, the first category includes public hospitals located in capitals of governorates, or in administrative centers with populations exceeding 500,000 people. The clinical capacity of the first category was set at 200 beds or more. The second category includes central hospitals of type “A”, serving administrative centers whose population ranges between 100,000 to 500,000 people. The second category puts their capacity at 100 to 199 beds.
The third category includes the central hospitals of type “B”. These are located in cities with less than 100,000 inhabitants, with a clinical capacity ranging from 50 to 99 beds. The fourth category covers “quality hospitals” that serve cities also with populations less than 100,000, with the number of beds ranging from 50 to 99 too.
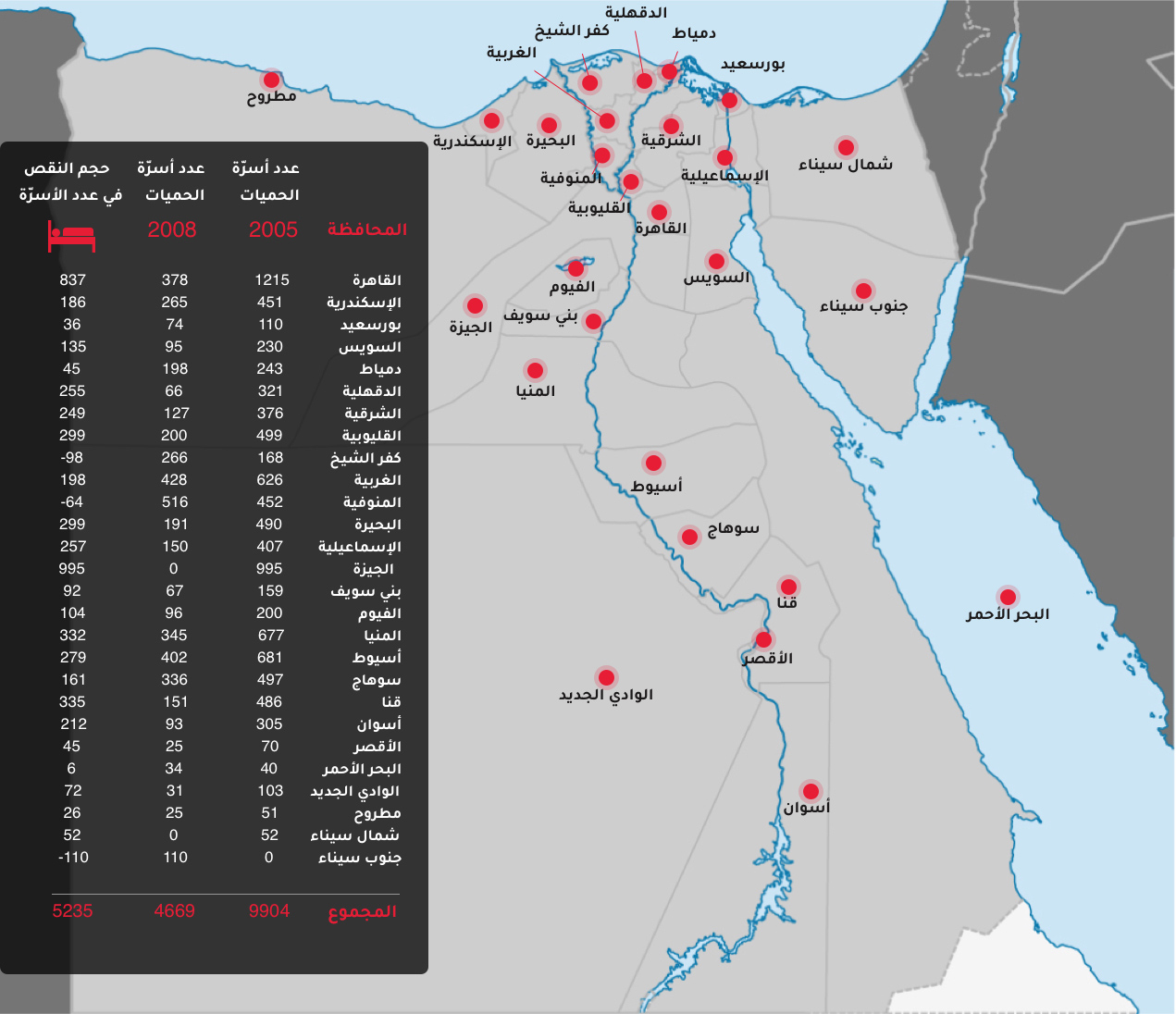
The fifth and sixth categories are similar to the first and second models of health facilities. These provide primary care and family health services, and are the first point of contact for citizens. These facilities provide 1,000 to 20,000 beds (depending on the area and its demography). Once this regulation was implemented, about 60 infection hospitals went out of service as they were turned into departments at central hospitals. Unfortunately, most of the infection hospitals or “Al Hemyat” are located in poor cities and villages; therefore, their affiliation with the central hospitals was changed from category “B,” leading to the elimination of around 5,235 beds.
By reviewing the annual health bulletin issued by the Central Agency for Public Mobilization and Statistics from 2005 to 2019, Arij has found that the number of beds in infection hospitals or “Al Hemyat” decreased from 9,904 in 2005 to 4,669 beds in 2019 –– marking a 50% drop.
 Al Qalyubia
El Beheira
Al Sharqiya
Dakahlia
Menofia
Kafr El Sheikh
Damietta
Al Qalyubia
El Beheira
Al Sharqiya
Dakahlia
Menofia
Kafr El Sheikh
Damietta

The hospital closed in 2010
Bahteim Hospital
The hospital closed in 2010
Kharkania Hospital
The hospital closed in 2010
Shebin El-Qanater Hospital:
The hospital closed in 2010
El Qanater Hospital
The hospital closed in 2010
Al-Khanka Hospital
The hospital was transformed in 2009
Delengat Hospital
Partial hospital closure in 2010
Al-Matamir Hospital
Shoubrakhit Hospital:
The hospital turned into a department of Shoubrakhit Central Hospital.
Kom Hamada Hospital:
The number of beds has been reduced
Rashid Hospital:
The number of beds has been reduced
Tahrir Hospital:
The number of beds has been reduced
Itay Al-Baroud Hospital:
The number of beds has been reduced
Minya Al-Qamh Hospital:
The number of beds has been reduced
Belbeis Hospital:
The number of beds has been reduced
Husseinieh Hospital:
The number of beds has been reduced
Ibrahimia Hospital:
The number of beds has been reduced
Hehia Hospital:
The number of beds has been reduced
The building has been worn out since 2010
Dikirnis Hospital
Manzala Hospital
The number of beds has been reduced
Mit Ghamr Hospital
The number of beds has been reduced
Shoubrahor Hospital
The number of beds has been reduced
Sherbin Hospital:
The number of beds has been reduced
Belqas Hospital:
The number of beds has been reduced
The hospital closed in 2010
Sadat Hospital
Zaweyat Al Naoura Hospital:
The number of beds has been reduced
Tala Hospital:
The number of beds has been reduced
Bella Hospital:
The number of beds has been reduced
Motobas Hospital:
The number of beds has been reduced
Zarqa Hospital:
The number of beds has been reduced
Faraskur Hospital:
The number of beds has been reduced
Beni Suef
Giza
Minya
Asyut
Sohag
Qena
Aswan
Ismailia
Luxor
It was transferred to a department of Al Wasiti Central Hospital in 2010
Grade Hospital: The number of beds has been reduced
A decision was issued to remove it in 2002 due to the building's wear and tear.
Al-Ayyat Hospital:
The number of beds has been reduced
Al Fashn Hospitals: The number of beds has been reduced
And it turned into a department of Al-Saf Central Hospital A in 2010
The number of beds has been reduced
Atfih Hospital:
The number of beds has been reduced
Al-Ayyat Hospital:
The number of beds has been reduced
Transferred to a department of Al-Fikriyah Central Hospital A in 2010.
The number of beds has been reduced
Transferred to a department of Dairout General Hospital in 2010.
The number of beds has been reduced
The number of beds has been reduced
Abu Tig Hospital: The number of beds has been reduced
Al-Ghanayem Hospital: The number of beds has been reduced
Al-Badari Hospital: The number of beds has been reduced
Dweir Hospital: The number of beds has been reduced
Transferred to a department of Gerga General Hospital in 2010.
The number of beds has been reduced
Tama Hospital: The number of beds has been reduced
Facility Hospital: The number of beds has been reduced
Akhmim Hospital: The number of beds has been reduced
Juhayna Hospital: The number of beds has been reduced
Belina Hospital: The number of beds has been reduced
Maragha Hospital: The number of beds has been reduced
Transferred to a department of Deshna Central Hospital A in 2010.
The number of beds has been reduced
Farshout Hospital: The number of beds has been reduced
Naqada Hospital: The number of beds has been reduced
Endowment Hospital: The number of beds has been reduced
Qeft Hospital: The number of beds has been reduced
Transferred to a department of Drau Central Hospital in 2010.
Drew Hospital: The number of beds has been reduced
The hospital was transferred to a department affiliated with Nasr El Nuba Central Hospital in 2010
Transferred to a department of Esna Central Hospital in 2010.
Esna Hospital: The number of beds has been reduced
Al-Qassaseen Fever Hospital: The hospital was closed and turned into a department inside Al-Qassasin Central Hospital B.
And it's still closed
Al-Tal Al-Kabeer Fever Hospital: Its construction cost about 31 million pounds since 2005
Moreover, the unified list made no mention of “Al Takamol” hospitals as they were listed in 1997 regulation and were identified as hospitals ran by a doctor who had previously worked in the (national) health service with a qualification higher than a bachelor’s degree, and was to be assisted by a sufficient number of doctors and technicians needed to perform medical and preventive services.
According to the report issued by the Ministry of Health in 2012, of which ARIJ obtained a copy, the number of “Takamol” hospitals in all governorates had reached 522. In 2016, the Ministry of Health was preparing to launch these in a partnership system with the private sector based on a suggestion from the former Minister of Health, Ahmad Imad.
Time passed slowly in front of the Health Insurance Hospital in Naser City. Basma spent it yelling at the security officers, begging them, “By the mercy of the Prophet, please put her on an oxygen machine, even if on a chair!”
All her attempts failed to open the hospital’s iron gate.
Due to the 2010 regulation, the number of public hospital beds decreased from 116,100 beds in 2005 to 95,700 beds in 2019. Reviews of data issued by the annual health bulletin of the Central Agency for Public Mobilization and Statistics, revealed that 20,500 beds had been eliminated.
In March 2011, the Minister of Health, Dr. Ashraf Hatim, issued order No. 344 to suspend the implementation of the 2011 unified list. This came after the toppling of the regime of former President Hosni Mubarak (1981-2011) following the January revolution. Even then, Hatim did not reinstate the axed beds.
Hatim, now the former Minister of Health, explained that his decision to suspend the unified list was based on recommendations by a committee that included infections and lungs related illnesses specialists.
In a phone call, he said the committee concluded that, in order to protect the country from epidemics and infectious diseases like bird flu or Covid-19, hospitals dedicated to infectious diseases must be preserved. The committee recommended that they be developed in anticipation of current and future pandemics.
Hatim says that a plan for development was setup, but execution did not take place due to the country’s changing political conditions. The plan remains neglected until now.


Moreover, Dr. Tarek Kamel, former secretary general of the Medical Syndicate Fund, confirms that Egypt has traditionally suffered from a shortage in beds in public hospitals compared to global population ratio standards.
In a phone conversation, he blamed that on the lack of financial capabilities, stating that “80% of a good health service depends on good funding, and only 20% is reliant on good management and recruitment.”
It is noteworthy that the budget allocated to the Ministry of Health did not reach 3% of Egypt’s gross national product, as stipulated by the 2014 Constitution. In fact, reviews of the Ministry of Health budgets for the past four years reveal that this percentage did not exceed 1.6% of the gross national product.

After an hour of crying and begging, Basma took her grandmother to the ‘Abbassia’ Fever Hospital, but the security officers intercepted her again. She explained that she contacted “everyone and anyone I know, until my grandmother was admitted to the hospital after much agony.”
Finally, more than 24 hours after Basma’s grandmother lost consciousness, they found her an empty chair in the corner of the hospital’s crowded reception hall.
The Egyptian Institute for Studies considers infection hospitals as the “first line of defence” to address infectious diseases and epidemics, including Coronavirus. These hospitals could be fully dedicated to quarantine COVID-19 patients.
A study published by the Institute last March states that infection hospitals suffer from a shortage in equipment, rendering them unable to receive COVID-19 patients. The Ministry of Health had designated about 370 quarantine hospitals, the 60 infection hospitals that were turned into departments were not amongst them.
The Institute explains that infection hospitals suffer from an “identity crisis,” due to the fluctuation of their affiliation between the curative and preventive medicine sectors in the Ministry of Health. This caused an imbalance in their structure in 2011, in which administrative responsibilities were relegated to the preventive sector and technical responsibilities to the curative sector. In 2017, the management of infection hospitals was fully transferred to the preventive sector.
It is noteworthy that the decision to transfer these hospitals to the preventive medicine sector led to a delay in joining the comprehensive health insurance system. This affected the future of these hospitals, leaving them out of the priority lists of development and efficiency enhancement programs.
Dr. Tarek Ali, deputy director of the ‘Abbassia’ Fever Hospital, says that doctors of infectious diseases are of those most vulnerable to infection because of the nature of their work in handling epidemics and operating in quarantined areas. However, their “infection allowance” ranges between 19 to 30 pounds, depending on the doctor's rank.
After a legislative amendment, President Abdel Fattah Al-Sisi decided to increase the risk allowances of medical professionals by 75%, from the current value to 1225 Egyptian pounds per doctor. The Egyptian Medical Syndicate, however, states that the net increase in the allowance after deductions would only range between 250 to 400 pounds.
In a phone call, Dr. Tarek Ali said that the limited salaries of doctors in infection departments, and the difficulty of registering their affiliation within the ministry, led to a reluctance of medical school graduates to join the department.
Egypt suffers from a general shortage of doctors; out of 212,835 physicians who have obtained a license to practice as per the Egyptian Medical Syndicate, only 82,000 –– 38% ––of them actually work in the country. According to a study prepared by the Supreme Council of Universities and the Technical Office of the Egyptian Ministry of Health, those that work either work in Ministry of Health-affiliated hospitals, university hospitals or in the private sector.
The study published in 2019 shows that 62% of those doctors work outside Egypt, have resigned from government work or obtained leave of absence from the government. This data confirms that the true ratio of doctors in Egypt stands at one doctor for every 1,162 individuals. The global average stands at one doctor per 434 individuals.

Once Basma’s grandmother settled on one of the reception chairs of ‘Abbassia’ Hospital, the nurse put a respirator mask on her. In the meantime, Basma bought a comforter and a blanket to keep her warm.
While Basma was submitting her information and phone number, she was surprised that the medical staff asked her to leave, claiming that the hospital only accommodates patients.
A study conducted by researchers from the University of Queensland in Australia in partnership with the Egyptian Ministry of Health shows that a reduction of health expenditures has forced citizens to increase their personal expenditures on treatment. This, in turn, led to inequality in accessing healthcare, leaving it only to those who can afford it.
The study, published in 2018, adds that the economic policies of the two former presidents, Anwar Sadat (1970-1981) and Hosni Mubarak (1981-2011), led to the privatization of the healthcare system.
A report issued by the 20/20 Cooperation Agreement for Health Systems funded by the United States Agency for International Development (USAID) shows that personal spending on health in Egypt increased from 51% in 1995 to 60% in 2008. The World Health organization (WHO), however, has estimated the latter percentage at 72%.
The report divides personal spending methods into nine areas: private clinics at 38.4%; followed by pharmacies at 33%; private hospitals at 8.2%; hospitals of the Ministry of Health at 3.5%; treatment centers at 2.9%; university hospitals at 2.8%; health insurance hospitals at 1.9%; then 0.9% over other public hospitals; and finally, 8.3% for other expenses.
The 2010 report recommends increasing public investment in the health sector and addressing the issue of out-of-pocket spending. It also considers continued out-of-pocket spending a heavy burden, and a matter of grave concern.
It calls to address the lack of efficiency in the current system by merging strategy and procedure into a single system. This should be designed to cover various population groups, and to link investments to disease burden and demographic trends. Currently, investments in health do not reflect the geographical distribution of disease burden –– whether caused by increasing rates of chronic diseases, or a rise in the demographic of seniors.
Ten minutes after Basma left the ‘Abbassia’ Fever Hospital, the receptionist called her to inform her of her grandmother’s death.